A Rare Case of Evans Syndrome Associated with Underlying Dermatomyositis Without Generalized Subcutaneous Edema: A Case Report
Brian Shaw1, Mohammad Karaman1, Rameez Rao2, Ryan Shaw3, Steve J Carlan4*
1Department of Internal Medicine, USA
2Department of Pulmonology, USA
3University of South Florida, Biomedical Sciences Department, Tampa, Florida, USA
4Division of Academic Affairs and Research, USA
*Correspondence author: Steve J Carlan, Division of Academic Affairs and Research, Orlando, Florida, USA; Email: [email protected]
Published Date: 31-12-2023
Copyright© 2023 by Carlan SJ, et al. All rights reserved. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
| Received 05 Dec, 2023 | Accepted 24 Dec, 2023 | Published 31 Dec, 2023 |
Abstract
Background: Primary Evans Syndrome is a typically idiopathic systemic illness associated with a number of autoimmune conditions and lymphomas and characterized by Coombs-positive warm-agglutinin Autoimmune Hemolytic Anemia (AIHA) and immune thrombocytopenia. The disease can be severe and prolonged with multiple recurring disease flares. Its association with dermatomyositis remains exceedingly rare and all reported cases have been accompanied by generalized subcutaneous edema.
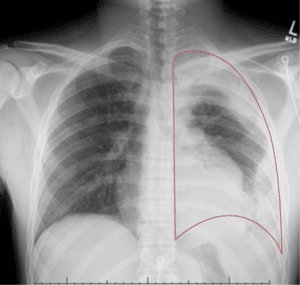
Case Report: We report a case of a 24-year-old male with a decade-long medical history of Evans Syndrome who presented to the emergency room with a one-week history of shortness of breath and fatigue. An extensive workup revealed severe anemia, thrombocytopenia and a left hemothorax. Active intervention included video-assisted thoracoscopy with decortication, blood products and autoimmune investigation. He was ultimately diagnosed with dermatomyositis after an electromyograph showed findings consistent with demyelinating peripheral polyneuropathy of motor nerves.
Conclusion: Evans syndrome associated with dermatomyositis is extremely rare and this is to our knowledge the first reported case of Evans syndrome associated with dermatomyositis without generalized subcutaneous edema.
Keywords: Evans Syndrome; Autoimmune Disease; Dermatomyositis; Hemolytic Anemia