Review Article | Vol. 6, Issue 2 | Journal of Dental Health and Oral Research | Open Access |
Rim Bourgi1,2,3*, Louis Hardan1,4, Carlos Enrique Cuevas-Suárez5, Nicolas Nassar4,6,7, Naji Kharouf2,8, Youssef Haikel2,8,9
1Department of Restorative and Esthetic Dentistry, Faculty of Dental Medicine, Saint-Joseph University of Beirut, Beirut 1107 2180, Lebanon
2Department of Biomaterials and Bioengineering, INSERM UMR_S 1121, University of Strasbourg, 67000 Strasbourg, France
3Department of Restorative Sciences, Faculty of Dentistry, Beirut Arab University, 115020 Beirut, Lebanon
4Department of Digital Dentistry, AI and Evolving Technologies, Saint-Joseph University of Beirut, Beirut 1107 2180, Lebanon
5Dental Materials Laboratory, Academic Area of Dentistry, Autonomous University of Hidalgo State, San Agustín Tlaxiaca 42160, Mexico
6Department of Orthodontics, Faculty of Dental Medicine Saint-Joseph University of Beirut, Beirut, Lebanon
7Craniofacial Research Laboratory, Faculty of Dental Medicine, Saint Joseph University of Beirut, Beirut, Lebanon
8Department of Endodontics and Conservative Dentistry, Faculty of Dental Medicine, University of Strasbourg, 67000 Strasbourg, France
9Pôle de Médecine et Chirurgie Bucco-Dentaire, Hôpital Civil, Hôpitaux Universitaires de Strasbourg, 67000 Strasbourg, France
*Correspondence author: Rim Bourgi, Department of Restorative and Esthetic Dentistry, Faculty of Dental Medicine, Saint-Joseph University of Beirut, Beirut 1107 2180, Lebanon and Department of Biomaterials and Bioengineering, INSERM UMR_S 1121, University of Strasbourg, 67000 Strasbourg, France and Department of Restorative Sciences, Faculty of Dentistry, Beirut Arab University, 115020 Beirut, Lebanon; E-mail: rim.bourgi@hotmail.com
Citation: Bourgi R, et al. Advances in Resin–Dentin Bonding: Evaluating Pre-Treatment Techniques for Improved Adhesion. J Dental Health Oral Res. 2025;6(2):1-32.
Copyright© 2025 by Bourgi R, et al. All rights reserved. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
| Received 07 July, 2025 | Accepted 21 July, 2025 | Published 28 July, 2025 |
Abstract
Achieving durable resin-dentin bonds has long been a focus in restorative dentistry. This review examines 16 strategies to enhance dentin adhesion, including the use of an additional layer of hydrophobic coating, extending application time, Non-Thermal Atmospheric Plasma (NTAP), Ethanol Wet-Bonding (EWB) and Acetone Wet-Bonding (AWB), multiple-layer applications, enhanced solvent evaporation using a warm air stream, prolonged curing time, extended air-blowing, the use of Matrix Metalloproteinase (MMP) inhibitors, crosslinking agents, electric current to improve monomer impregnation, field control, selective dentin etching (SDE), enhanced dentin impregnation using a scrubbing technique, biomimetic remineralization, dentin pre-treatment with Airborne Particle Abrasion (APA) or Dimethyl Sulfoxide (DMSO). Inclusion criteria for the studies focused solely on dentin, with no time restrictions. Results indicate that clinicians may need to modify application protocols, deviating from the manufacturer’s recommendations, to improve the Bond Strength (BS) of resin-based materials to dentin. The application modalities that enhanced BS to dentin included the use of a hydrophobic resin layer, double adhesive application time, NTAP, EWB, AWB, multiple adhesive layers (two or more), warm air stream on the primer or adhesive system (gold standard around 50 and 60°C), curing time extended to 40 s, prolonged air-drying, prior application of MMP inhibitors, crosslinking agents, electric current-assisted application, appropriate isolation with a rubber dam, SDE for 3 s, scrubbing technique, biomimetic remineralization, APA in specific adhesion strategies and the use of DMSO. The outcomes demonstrate that these strategies, when properly executed, can lead to improved adhesive performance and long-term durability. Notably, no single method outperformed all others, but a combination of these strategies can optimize BS. The review concludes that achieving reliable and durable resin-dentin bonds require tailored application modalities, a deeper understanding of adhesive chemistry and innovation in clinical techniques to improve the longevity of dentin restorations.
Keywords: Adhesive-Dentin Interface; Adhesive Systems; Dentin; Dentin Bonding
Introduction
In restorative dentistry, adhesive systems have transformed clinical approaches, enabling restorations without mechanically retentive cavities by providing immediate Bond Strength (BS) and reliable sealing capabilities [1,2]. While enamel bonding is predictable and durable, dentin bonding is more complex due to the material’s heterogeneous and hydrophilic nature. This complexity makes the creation of a long-lasting, stable bond more challenging [3,4].
There are currently two primary bonding techniques for dentin: the Etch-and-Rinse (ER) technique, which separately etches dentin before adhesive application and the Self-Etch (SE) technique, where etching and priming are combined [5,6]. Both methods aim to create a strong, durable “Hybrid Layer” (HL), a structure composed of demineralized collagen fibrils reinforced with infiltrated resin [7]. Universal Adhesives (UAs), which integrate both ER and SE techniques, have increased bonding versatility by enabling selective etching on enamel and self-etching on dentin. This approach streamlines clinical procedures and adapts to diverse restorative needs [8,9].
The formation and quality of the HL-comprising dentin collagen, infiltrated resin monomers, residual Hydroxyapatite (HAp) and solvents-are crucial for the durability of the resin-dentin bond [10]. Despite 50 years of advancements in adhesive technology, maintaining a stable interface remains a challenge. Hydrolytic degradation and enzymatic activity-particularly from Matrix Metalloproteinases (MMPs)-can gradually weaken the HL, destabilizing the bond and degrading unprotected collagen fibrils [11,12]. This ongoing degradation is partly due to factors such as residual moisture, which affects resin monomer penetration and Nanoleakage (NL), both of which reduce the longevity of resin-dentin bonds [13,14].
To address the durability challenges associated with dentin bonding, various strategies have been investigated to improve the longevity of adhesive systems. These include the use of crosslinking agents for collagen biomodification, hydrophobic adhesive formulations and MMP inhibitors such as Chlorhexidine (CHX) [15,16]. Recent advancements also involve applying antibacterial agents to prevent biofilm formation, utilizing nanofillers to enhance the mechanical characteristics of adhesives and optimizing moisture control during bonding procedures [17,18]. Furthermore, effective techniques for facilitating solvent removal and enhancing adhesive durability have been identified. These techniques include prolonged air-drying, applying warm air to the primer or adhesive system extending application times, active bonding application, multiple adhesive layers, an additional hydrophobic coat and extended light-curing exposure [19,20].
While various approaches may be introduced by clinicians to improve BS, a universally accepted protocol for achieving optimal adhesion to dentin remains elusive [21-23]. Nonetheless, a rise in BS is achievable through numerous strategies, as supported by many authors [22,23].
Moreover, biocompatibility is a critical requirement for dental adhesives, given their prolonged contact with vital dentin [24]. Methacrylate monomers (i.e., Bisphenol A Glycidyl Methacrylate (Bis-GMA), Urethane Dimethacrylate (UDMA) and 2-Hydroxyethyl Methacrylate (HEMA)) have been described to produce toxicity, including Glutathione (GSH) depletion, cell cycle arrest and apoptosis/necrosis in human gingival fibroblasts [25,26]. It is well documented that HEMA can lead to morphological changes and growth suppression in various cell types [27,28]. One possible explanation for the adverse impacts of dentin adhesives is the leakage of resin monomers [29]. Therefore, establishing the gold standard method for placing adhesive systems to dentin should guarantee that the material is converted to the maximum extent possible.
This review aims to critically evaluate the most recent interventions and innovative approaches aimed at enhancing the longevity and stability of resin-dentin bonds in restorative dentistry. It will examine various pre-treatment strategies, adhesive formulations and novel materials that contribute to improved adhesion, offering insights into their effectiveness in mitigating common challenges such as hydrolytic degradation and bond failure over time [22,23,30].
Methodology
This narrative review was conducted to explore and synthesize existing evidence regarding strategies aimed at improving resin-dentin bonding. Unlike systematic reviews, which follow strict protocols for study selection and appraisal, narrative reviews allow for a broader and more flexible inclusion of literature to provide a comprehensive understanding of a topic.
The literature search was performed using reputable scientific databases including PubMed, Scopus, Web of Science and Google Scholar. Studies were included if they focused on dentin bonding with resin-based materials and presented experimental or clinical data on techniques or materials designed to enhance BS or durability. No time restrictions were applied.
To ensure the reliability and scientific quality of the information discussed, preference was given to articles published in peer-reviewed journals with established scientific rigor, higher impact factors and high citation counts. This criterion was used to prioritize studies that have demonstrated relevance and influence within the academic community. While this approach may have excluded some emerging or less-cited literature, it was adopted to strengthen the credibility of the conclusions drawn.
Non-peer-reviewed articles, conference abstracts, opinion pieces and studies lacking sufficient methodological detail were excluded. The final selection reflects a representative and influential body of evidence on current and emerging strategies in resin-dentin bonding.
Dentin Versus Enamel: Structural and Adhesive Challenges
The primary goal of adhesive restorations is to achieve a durable bond with sufficient mechanical properties while maintaining a lasting seal to enamel and dentin [31]. Bonding to enamel is relatively straightforward, as it relies on micro-mechanical interlocking of Resin Tags (RTs) within the microporosities created by acid etching. This mechanism effectively seals restoration margins against leakage. However, bonding to the more organic and humid dentin substrate presents significant challenges in adhesive dentistry [32,33].
Enamel, a highly mineralized tissue, is composed of 96% inorganic material and 4% organic matter and water. Its structure consists of long, parallel apatite crystals configured into enamel rods with a decussating pattern [34]. In contrast, dentin has a more complex composition, with 70% inorganic carbonated calcium phosphate microcrystals, 20% organic matrix and 10% water [35].
The dentin organic matrix is predominantly type I collagen, forming approximately 90% of its structure. The collagen matrix provides a fibrous three-dimensional framework essential for dentin’s resilience and ability to remineralize [36]. Dentin also includes odontoblast processes, which extend from cells lining the pulp chamber into the mineralized dentin, traversing through dentinal tubules. These tubules are smaller and fewer in number near the enamel-dentin junction compared to the pulp interface [37,38].
Structurally, dentin’s smaller, less systematically oriented crystallites offer increased surface area, making it more susceptible to acid attack [39,40]. In addition, the dentin tubules and their surrounding collagen matrix present significant challenges for achieving a durable adhesive bond due to moisture content, enzymatic degradation and variations in substrate preparation [41].
Understanding these inherent differences between enamel and dentin is crucial for advancing adhesive strategies, as the complex composition and structure of dentin require more sophisticated approaches to achieve effective and long-lasting restorations. These complexities contribute to higher clinical failure rates in dentin bonding. Restorations involving dentin are more susceptible to issues like marginal leakage, recurrent caries and debonding, especially in high-stress regions. Studies have shown that dentin bonds degrade faster than enamel bonds due to the combined effects of hydrolysis, enzymatic activity and polymerization shrinkage [31,32]. Thus, this study seeks to address these challenges by exploring advanced adhesive technologies and strategies aimed at improving resin-dentin bond durability.
Classification of Adhesives
In dentistry, adhesives are categorized based on their functional roles and clinical applications. Adhesives are engineered to withstand mechanical stresses and ensure robust, long-lasting bonds in restorative and rehabilitative treatments. These adhesives operate via several mechanisms, including micro-mechanical interlocking, chemical bonding and dispersive adhesion. Micro-mechanical adhesion occurs as the adhesive penetrates surface irregularities, such as etched enamel prisms or demineralized dentin (Fig. 1), to create a mechanical anchor.

Figure 1: Adhesive interlocks into the etched dentin to form the hybrid layer, also known as the interdiffusion layer, which serves as the primary mechanism of adhesion (courtesy of Prof Carlos Enrique Cuevas-Suárez).
For example, the ER adhesive systems leverage phosphoric acid to remove the smear layer, exposing the underlying tooth structure and enabling deep adhesive infiltration. These systems are renowned for high BS and durability but are technique-sensitive and require precise moisture control to avoid collagen collapse or over-etching [42-44]. Conversely, SE adhesives simplify the process by combining etching and priming into a single step, reducing clinical errors. These systems rely on functional monomers like 10-methacryloyloxydecyl dihydrogen phosphate (10-MDP), which chemically bond to calcium in HAp through ionic interactions. The formation of a stable nano-layer further enhances durability and resistance to hydrolysis. Other examples of structural adhesives include glass ionomer cements, which rely on polyalkenoic acids to form ionic bonds with calcium and adhesive resins used in fiber-reinforced restorations, where mechanical and chemical interactions work synergistically [45-50].
Advances in dental adhesive systems, including the introduction of UAs, have blurred these distinctions, allowing for more versatile and effective solutions [51,52].
Chemistry of Contemporary Dental Adhesive Systems
A dental adhesive system consists of several fundamental components. The etchant, typically phosphoric acid (H3PO4), is commonly used at a concentration ranging from 30% to 40%. To enhance the precision of application and ensure complete removal, H3PO4 gels are thickened using silica microparticles, with alternative thickeners like xanthan gum also being incorporated. To further improve application, a color dye is added, making it easier to observe the area being treated. Glycol is frequently included to enhance wettability and reduce viscosity. After application, the etchant is completely washed off the dental surface [53-55].
The primer is a hydrophilic solution containing resin monomers, an organic solvent (such as alcohol or acetone), water and stabilizers [56]. The hydrophilic groups in the primer enhance the wettability of dentin, which is crucial in the humid oral environment. In terms of function, primers serve a role like that of paint in surface preparation, forming a bonding layer that prepares the dentin for the bonding resin by facilitating adhesion [53]. HEMA is the most used primer due to its high hydrophilicity and solvent-like properties [57]. Typically, primers are neither washed nor cured after application to the tooth surface; instead, they are air-dried [53].
The bonding resin, which is a low-viscosity, solvent-free (hydrophobic) resin, is placed over the primer and then polymerized. The hydrophobic groups in the bonding resin engage and copolymerize with the restorative material, enhancing the stability and durability of the resin-dentin bond by effectively sealing the bonded interface against NL [53]. The hydrophobic resin also increases the polymerization rate of the primer and improves the mechanical properties of both the adhesive and the HL [53,58]. Adhesive systems that incorporate a separate bonding phase generally provide superior results. These bonding resins are typically composed of hydrophobic dimethacrylates such as Bis-GMA, Triethylene Glycol Dimethacrylate (TEGDMA) and UDMA [53,59].
In addition to these basic components, adhesive systems may contain other ingredients, such as initiators. For self-cure resin systems, an initiator like benzoyl peroxide can trigger polymerization, while photo-initiator systems with photosensitizers (e.g., camphorquinone) and activators (e.g., tertiary amine) are commonly used in light-cured systems. Fillers like silica particles are often included and other additives may serve specific functions, such as paraben for antimicrobial activity, Glutaraldehyde (GA) as a desensitizer, fluoride to help prevent secondary caries and CHX to inhibit collagen degradation [57,60].
Overall, the chemistry of a dental adhesive system is summarized by the formula M-R-X, where “M” represents a methacrylate group that bonds with the resin matrix, “R” is a spacer and “X” is a functional group that facilitates adherence to dental surfaces [61].
Adhesion Phenomena in Dentistry: A Materials Science Perspective
Adhesion refers to the ability of dissimilar surfaces or particles to bond and it is a fundamental concept in dental materials science. This bonding can be categorized into three principal types: chemical adhesion, dispersive adhesion and diffusive adhesion, each contributing uniquely to the overall adhesion phenomenon.
Chemical adhesion involves the formation of strong chemical bonds, such as ionic or covalent bonds, between the adhesive and the substrate. In dentistry, this is exemplified by the interaction of carboxylate-based luting agents with calcium ions in HAp. However, such interactions are limited to specific material combinations and are often vulnerable to degradation in moist oral environments [62-64].
Dispersive adhesion, driven by weak intermolecular forces like van der Waals interactions, plays a more generalized role. Although these forces are weaker than chemical bonds, they contribute significantly to adhesion strength when combined with other mechanisms [65].
Diffusive adhesion, on the other hand, arises when adhesive molecules penetrate the substrate at a microscopic or molecular level, promoting a strong bond through physical entanglement and interdiffusion [66]. In addition to these primary mechanisms, micro-mechanical adhesion is pivotal in dental applications. It occurs when adhesives infiltrate surface irregularities created by processes such as etching. This mechanism is particularly evident in resin-based adhesives, providing mechanical retention and resistance to stress [67-69].
From a materials science perspective, the success of adhesive bonding in dentistry depends on several factors, including surface preparation adhesive composition and polymerization behavior [70-76]. Adhesion in dentistry is thus a multifactorial process, requiring the integration of mechanical and chemical principles to achieve durable and effective bonding. Continued advancements in adhesive technologies, such as the development of UAs and the incorporation of nanomaterials, are addressing long-standing challenges like hydrolysis and mechanical fatigue, ensuring improved clinical outcomes [73,75].
Advances in Adhesive Monomer Technologies
Recent advancements in adhesive technology have had a profound impact on restorative dentistry, enabling strong and durable bonding between dental materials and tooth tissues [77-80]. The latest development in adhesive technology is the universal adhesive, which offers versatility and simplicity [60,81]. These systems are compatible with ER, SE and selective-etch techniques. They often incorporate functional monomers such as 10-MDP, known for forming stable chemical bonds with calcium in HAp. This bond creates a durable interface resistant to hydrolysis and enzymatic degradation, enhancing the longevity of the adhesive interface [82].
The 10-MDP monomer was patented by Kuraray Noritake, and it is widely used in several universal adhesive formulations, including All-Bond Universal (Bisco, Inc., Schaumburg, IL, USA), Adhese Universal (Ivoclar Vivadent, Schaan, Liechtenstein) and Scotchbond Universal (3M ESPE, St. Paul, MN, USA) [83]. 10-MDP has been shown to outperform other functional monomers in terms of chemical bonding potential, forming stable nano-layered structures that enhance hybridization and BS [84,85]. The self-assembly of 10-MDP into nano-layers involves the deposition of 10-MDP-Ca salts, creating a stable interface that resists degradation and enhances the overall durability of the bond [86]. The unique characteristics of 10-MDP, including its hydrophobic nature and its ability to reduce water sorption, contribute to its superior performance in dental adhesive systems [87,88].
Glycerol-Phosphate Dimethacrylate (GPDM) Monomer: Another recent advancement in adhesive monomers is the incorporation of GPDM, which combines both hydrophilic and hydrophobic properties [89]. GPDM facilitates wet-bonding to dentin while ensuring polymer matrix stability. It also forms ionic interactions with calcium ions, promoting a stable HL at the adhesive interface [59]. Studies have demonstrated that GPDM-containing adhesives offer improved BS and durability, especially under challenging oral conditions [59,90]. Unlike 10-MDP, GPDM does not expose collagen during bonding but promotes the formation of a thick HL with exposed collagen, contributing to the bonding effectiveness [59,91]. The interaction of GPDM with co-monomers and its effects on bonding durability warrant further investigation.
Dipentaerythritol Pentaacrylate Phosphate (PENTA-P) monomer is another notable monomer in modern adhesives. This monomer is characterized by its five vinyl groups and shorter carbon chains compared to 10-MDP. This structure provides PENTA-P with superior resistance to hydrolytic degradation. Studies have shown that PENTA-P-based adhesives maintain stability even after prolonged shelf-life, making them more resilient than adhesives containing 10-MDP [89,92,93].
The progression from traditional three-step ER formulations to SE and UAs highlights the application of advanced materials science principles in dentistry. SE adhesives simplify the bonding process by combining etching and priming steps, while UAs offer clinical flexibility, allowing for a range of techniques based on specific needs [77].
Despite these innovations, challenges such as hydrolytic degradation of the adhesive interface continue to affect long-term performance. Factors such as collagen fibril breakdown and resin matrix degradation compromise BS. Strategies to address these issues include the incorporation of nanoparticles to enhance the resin matrix, the use of crosslinking agents to stabilize collagen and modifications in monomer chemistry to improve hydrophobicity [94,95].
The integration of advanced monomers like 10-MDP, GPDM and PENTA-P demonstrates the dynamic nature of adhesive research, where chemical innovation and clinical demands converge to create durable and effective solutions for modern dentistry [90,91,96].
Degradation Mechanisms of Resin-Dentin Bonds: Implications for Adhesive Performance
The main factor threatening the resin-dentin bond’s endurance is the HL’s gradual deterioration, which underpins the adhesive interface by integrating resin monomers with dentin collagen. This HL is composed of collagen fibrils, HAp, resin monomers and residual solvents, whose stability is crucial for maintaining BS over time (Fig. 2).

Figure 2: Scanning electron micrograph of the hybrid layer and resin tags: The proper adhesive way application (courtesy of Prof. Naji Kharouf).
The degradation mechanisms involve hydrolytic breakdown of the adhesive resin within the interfibrillar spaces and the disorganization of collagen fibrils due to water infiltration, enzymatic activity and occlusal stresses. The dentin’s intrinsic moisture and the hydrophilic nature of modern adhesives enable water to permeate the HL, initiating hydrolysis and leaching of resin adhesives, leading to phase separation and mechanical wear over time. Specifically, the degradation of adhesive resins is exacerbated by hydrophilic monomers, which absorb water and permit its movement across the resin-dentin interface, accelerating degradation and weakening BS [97-100].
To study the hydrolytic degradation mechanisms, in-vitro aging studies are commonly employed, where adhesive systems are subjected to simulated oral conditions, such as moisture and temperature fluctuations. These studies help quantify the effects of hydrolysis over time by evaluating changes in BS and resin composition, with particular attention to phase separation between hydrophilic and hydrophobic monomers within the HL [101,102].
Microscopic techniques such as Scanning Electron Microscopy (SEM) and Transmission Electron Microscopy (TEM) have been used to observe structural changes in the HL caused by water infiltration and enzymatic activity. These imaging methods reveal the disorganization of collagen fibrils and erosion of resin layers, visualizing the physical and chemical breakdown of the resin-dentin interface [103,104]. Additionally, in situ studies, which monitor real-time degradation under wet conditions, assess the role of enzymatic breakdown by MMPs in hydrolytic degradation. This combination of water and enzymatic activity accelerates the breakdown of collagen fibrils, leading to a weakened BS [105,106].
Chemical analysis methods such as Fourier-Transform Infrared (FTIR) spectroscopy are also employed to study changes in resin composition and identify degradation by-products resulting from hydrolysis. These analyses help elucidate the chemical interactions between water molecules and hydrophilic monomers, shedding light on their role in the degradation of adhesive systems [94].
Strategies to counter this phenomenon include using alternative hydrophilic photo-initiators, such as Trimethylolpropane Oxide (TPO), alongside traditional Camphorquinone (CQ) to increase the degree of cure of hydrophilic monomers and reduce phase separation risks [107,108]. Concurrently, incomplete resin infiltration into demineralized dentin leaves collagen fibrils exposed to water and endogenous collagenolytic enzymes, such as MMPs and cysteine cathepsins. These enzymes, part of the dentin “degradome,” play an active role in bond degradation by targeting collagen fibrils left unprotected due to partial adhesive penetration (Fig. 3) [109,110].

Figure 3: Scanning electron micrograph of the incomplete resin infiltration due to hydrolytic degradation: The improper adhesive way application (courtesy of Prof. Naji Kharouf).
Influence of Pre-Treatments and Outlook for a New Alternative in Resin-Dentin Bonding
To maximize performance and long-term outcomes of adhesive systems several strategies are reported:
Use of an Additional Layer of Hydrophobic Coating
Due to the hydrophilic nature of many adhesive monomers, the resin-dentin interface is vulnerable to water absorption, which negatively affects bond durability. Applying an additional hydrophobic adhesive layer has been shown to enhance the adhesive film’s thickness and polymerization, reducing water sorption and improving interface stability [111-113]. An alternative strategy involves using a flowable composite atop a thin adhesive layer. This serves as a stress absorber, especially beneficial in deep proximal boxes, improving marginal adaptation [114-116]. Since SE adhesives are generally more hydrophilic than ER systems, the use of an extra hydrophobic layer becomes even more critical with SE adhesives [117-119]. Studies have confirmed that applying an additional hydrophobic layer improves BS and reduces NL across different UAs when used in SE mode [120-125].
Application Time
A prior review found that decreased application periods reduced the BS of SE adhesive solutions [23]. Nowadays, clinicians are beginning to escalate step reduction settlements in both ER and SE adhesives [126,127]. The recently introduced adhesive system G-Premio Bond Universal (GC, Tokyo, Japan) offers dental clinicians an alternative to the SE strategy for dentin adhesion. According to the manufacturer’s instructions, it can be used without a waiting period for interaction with the bonding substrate (“no-waiting SE,” Japanese version) or with a 10-s wait time to allow interaction (“10-s SE,” international version) [128]. This innovative idea of a no-waiting adhesive, while pleasing to many clinicians, should not hinder the durability and performance of adhesives when bonding to dentinal substrate. It was established that the no-waiting SE strategy preceding adhesive photopolymerization may give adequate BS. Nonetheless, extended application times when using the 10s SE mode instead of the no-waiting mode enhance its short-term dentin bond performance [129]. As a result, applying an SE adhesive for a shorter duration than advised by the supplier may not be the optimum usage of the adhesive. Dentists typically work without using a watch to exactly record separate application procedures and they expect a reduction in their patients’ discomfort treatment times. Therefore, dentists may not always adhere strictly to manufacturers’ suggested application times, theoretically affecting dentinal BS and compromising the long-term durability of dental restorations [130,131]. As revealed by Hardan, et al., a shorter application time reduces the BS of UAs to dentin using both ER or SE modes [22]. Consequently, clinicians should not implement this adjustment. Extending the application duration of adhesives improved the chemical reaction of functional monomers and HAp, a key step for enhancing monomer infiltration (Fig. 4).

Figure 4: Extended adhesive time application of G2-Bond Universal (GC Dental Products, Kasugai, Japan) has been shown, via scanning electron microscopy, to produce an optimal hybrid layer and well-formed resin tags, ensuring effective adhesion and improved bonding to the dentinal substrate (courtesy of Dr. Rim Bourgi).
Dentin bonding can be enhanced through treatment with Non-Thermal Atmospheric Plasma (NTAP). While NTAP has been shown to improve aged BS, it does not significantly influence immediate BS. Plasma, described as partially ionized gases containing electronically excited atoms, molecules, ions and free radical species, is recognized for its ability to enhance bonding to dentin [132,133]. These reactive particles act as crosslinkers, forming chemical functional groups on the dentin surface [132]. NTAP treatment has demonstrated benefits such as promoting dentin wettability enhancing resin polymerization and improving resin infiltration [134-138]. Additionally, NTAP stimulates the dentin substrate by generating free radicals or peroxides, which intensify the interaction between collagen fibrils and resin monomers [139]. Moreover, Matrix Metalloproteinase-2 (MMP-2) and MMP-9 are naturally occurring MMPs in dentin. These enzymes may break down the collagen matrix within dentin over time, thus affecting the durability of resin-dentin connections. Accordingly, lowering the expression and activity of MMP-2 and MMP-9 may be favorable for improving the durability of resin-dentin bonds [140,141]. The previously indicated reduction in MMP-2 and MMP-9 expression and activity might perhaps be achieved by using NTAP on thyroid papillary carcinoma cells, suggesting a possible therapeutic impact of NTAP in lowering MMP activity and thereby increasing resin-dentin bonding [137,138,142]. Nonetheless, it has been proven that Microtensile Bond Strength (μTBS) and fracture-toughness testing have not consistently shown that dentin plasma therapy improves ER and SE bonding. Therefore, this method should not be considered effective enough [57].
Incorporating NTAP into clinical workflows presents some challenges. One significant barrier is the cost and complexity of the equipment needed to generate NTAP. Additionally, the potential risks of using plasma on sensitive dental tissues, such as unexpected thermal effects or insufficient control over the plasma’s intensity, require thorough management and training. Moreover, integrating NTAP into standard procedures could increase treatment times and demand additional procedural steps, impacting clinical efficiency [143]. Further studies and clinical trials are needed to assess its feasibility and optimize its application in dental bonding.
Ethanol or Acetone Wet-Bonding
The technique of Ethanol Wet-Bonding (EWB) relies on the ER bonding strategy, with the goal of totally replacing water with ethanol within the exposed collagen-fibril network. Employing the EWB approach helped in improving the immediate BS. Ethanol is a favored solvent over water because it can decrease the width of collagen fibrils while increasing interfibrillar space, allowing monomers to easily permeate the collagen fibrils [144]. In this simplified procedure, 100% ethanol is applied, which is safe for clinical use. When collagens are effectively preserved with ethanol, the adhesive interface exhibits prolonged durability, leading to a stable bond over time [145,146]. Other studies, however, reported that although this method is probably the most successful for improving ER bonding, it is not clinically practicable due to the time required for subsequent ethanol administrations (at least several min) [147,148]. Because ethanol has a higher viscosity compared to acetone, dental adhesives with acetone are less viscous, allowing acetone to penetrate the demineralized dental collagen matrix more effectively.
The Acetone Wet-Bonding (AWB) procedure has shown potential to maintain BS over extended periods. This technique offers a novel approach to enhancing dentin wettability for dental adhesives, improving adhesive monomer penetration, reducing collagen exposure, decreasing NL and minimizing collagen degradation [149]. Consequently, AWB emerges as a promising strategy to extend the longevity of adhesive restorations [149,150]. However, further research is required to validate the long-term efficacy of this technique (AWB).
Multiple-Layer Applications
Applying double or triple adhesive layers with simplified adhesive systems is recommended to enhance their performance [151]. It is important to note that adhesives containing fillers in their composition create a thicker adhesive layer compared to non-filled adhesives [152]. Adhesives with increased thickness (by several coats) were applied on dentin in a study by Zecin-Deren, et al., in 2019 where one layer, two layers and three layers were applied using four adhesives: two UAs and two SE ones [151]. The authors found that for Xeno V and Prime&Bond One Select (Dentsply DeTrey GmbH, Konstanz, Germany), a noticeable rise in adhesive layer thickness was observed, along with significantly higher BS. Such findings were not observed for Adper Easy One and Single Bond Universal (3M ESPE Dental Products, St. Paul, MN, USA). According to this study, the fillers inside these two adhesives (based on their specific compositions) produced a thicker adhesive layer. One should assume that the exact application protocol is dependent on the product [151].
Filler load or percent mass load, differs between adhesives according to the manufacturer’s technology and it is not well described in the composition of adhesives. Also, there is a matter of concern about the shrinkage of these filled adhesives after polymerization [153]. It was proven that the inclusion of nanofillers in the formulation of adhesive does not ensure a higher BS in comparison to unfilled adhesive systems [154]. Fillers may increase the viscosity of adhesives and prevent their overthinning, which can provide a thicker adhesive layer and function as an elastic buffer. If that adhesive layer is too thin, the polymerization process might not completely progress due to the oxygen inhibition phenomenon and this could result in reduced mechanical properties of the adhesive layer [155].
Nevertheless, it has been suggested that increasing the percentage of fillers or nanofillers could decrease the infiltration of adhesive to demineralized dentin and hence generate a defective HL [156].
Similarly, Fujiwara, et al., observed that the application of two layers of UAs (Prime&Bond Elect (Dentsply Caulk, Milford, DE, USA) and Scotchbond Universal (3M ESPE Dental Products St. Paul, MN, USA)) instead of one layer improved the adhesive quality, enhanced BS, produced a more uniform adhesive layer and compensated for possible defects of single application [157]. Zecin-Deren, et al., recommended using triple adhesive layers with simplified adhesive systems to increase their performance while focusing on the point that achieving a more reliable bond to dentin and hence maximum efficiency necessitates a specific protocol for each adhesive [151]. Fujiwara, et al., recommended using double adhesive layers with single-step adhesive systems, including universal ones [157].
Further, a preceding study found that employing this application increased immediate dentin BS but did not improve BS following aging [22]. Current bonding trends appear to prefer a single application of adhesive solutions, although this cannot result in a thicker HL or adhesive layer with micro-mechanical retention to the underlying composite resin. However, prior research suggested that double or triple adhesive coats improve dentin BS by increasing monomer diffusion into the HL and chemical interactions [158,159]. As a result, an additional layer of application should be regarded as a crucial clinical step. Moreover, it must be highlighted that the increased dentinal BS with double application is the effect of many mechanisms operating simultaneously. As the solvent within adhesives evaporates between each layer application, the concentration of co-monomers remaining increases thereby enhancing the quality of the HL [160,161]. So, based on what was established about multiple-layer applications (Fig. 5), clinicians might apply a double coat while examining the material and substrate contents of each adhesive [23].![]()
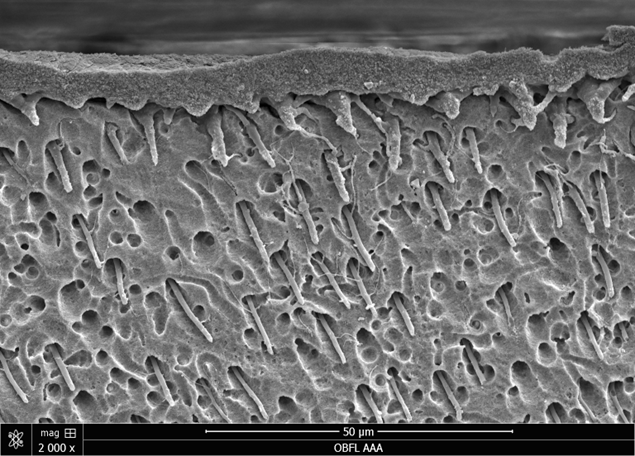

Figure 5: A representative scanning electron microscopy image of OptiBond FL (Kerr Corporation, Orange, CA, USA) demonstrates effective hybrid layer formation when three coats of active adhesive are applied to the dentinal substrate. This technique ensures optimal infiltration of the adhesive into the demineralized dentin, resulting in superior hybridization and enhanced bonding efficacy (courtesy of Dr. Rim Bourgi) [162].

Figure 6: A representative scanning electron microscopy image of OptiBond FL (Kerr Corporation, Orange, CA, USA) illustrates effective hybrid layer formation achieved by applying a 60°C warm air stream to the dentinal primer. This technique facilitates complete solvent evaporation, prevents residual solvent on the dentin surface, promoting superior hybridization and enhanced bonding efficacy (courtesy of Dr. Rim Bourgi).
Prolonged Curing Time
Increasing the photo-activation time improved the strength of both immediate and aged BS. Ideally, a restorative material must apply sufficient energy to transform monomers into stable polymers [22]. To increase polymerization (degree of conversion) and decrease permeability, extending the time of light exposure of adhesives beyond the manufacturer’s recommendation was preferred (i.e., from 20 s to 40 s to 60 s) [180]. In 2014, Wambier, et al., showed that reducing the sorption of water and the solubility of the adhesives is controlled by extending the time of light exposure of the adhesives [181]. While in 2011, Ferreira, et al., proved that an exposure time longer than what is recommended (20 and 40 s instead of 10 s) increases the degree of conversion of simplified adhesives (Adper Single Bond 2 (3M ESPE, St. Paul, MN, USA) and One Step Plus (Bisco, Inc., Schaumburg, IL, USA)) and the resin-dentin BS, but does not decrease NL [182]. In addition, it was previously demonstrated that an extension of the exposure time during light-curing improves the quality of the resin-dentin interface [183]. Likewise, in 2019, Cadenaro, et al., suggested that the degree of conversion of adhesives in deep class II cavities might increase when extending the exposure curing time to approximately 40 s-60 s [184]. On the other hand, they pointed out that damage to the pulp may occur because of heat generation from light-curing. The same findings were observed by Cadenero, et al., in 2005 and Breschi, et al., where they suggested that, even below ideal laboratory conditions and longer exposure times, the exposure time proposed for adhesive systems is not sufficient to obtain an optimal polymerization [185,186].
Therefore, prolonging photopolymerization of the adhesive guarantees an adequate degree of conversion; despite this fact, one should bear in mind that even Light-Emitting Diodes (LEDs), which were initially cold lights, produce heat up to 93% of their total energy. To solve this issue, the tooth should be air-cooled on an interval of 1 to 2 s after every 10 s of light exposure [184,187]. According to a prior meta-analysis, prolonged curing time for UAs reduces the adhesive’s susceptibility to water sorption and may keep the CQ in a state that permits it to react with a co-initiator, resulting in an elevated energy density and amplified free radical production [22,188]. In this case, the exposure time specified by the manufacturer for adhesive systems is insufficient to achieve adequate polymerization [185].
Prolonged Air-Blowing
In the bonding procedure, air-drying is a critical step following the application of the adhesive. Ethanol and water can form hydrogen bonds with each other and with the monomer, making it more challenging to remove water from ethanol-based adhesives compared to acetone-based adhesives [166]. As a result, it was anticipated that the effects of air-blowing time would be more pronounced for ethanol-based adhesives. A previous study found that longer air-blowing time significantly increased the BS of ethanol-based adhesives (Clearfil Universal (Kuraray Noritake, Tokyo, Japan) and Scotchbond Universal (3M ESPE, St. Paul, MN, USA)) after 24 h and 1 year. However, the BS of acetone-based adhesives (G-premio Bond (GC, Tokyo, Japan)) was unaffected by different air-blowing times.
Generally, the recommended air-blowing duration for newer UAs ranges from 5 to 15 s or until the liquid film on the surface becomes immobile. However, the specific air-blowing time is not standardized [189]. Prolonged air-blowing, from 5-10 s to 15-30 s, has been suggested to enhance the immediate adhesive properties of some UAs [190]. Furthermore, prolonged or strong air-blowing of HEMA-free adhesives resulted in higher BS and fewer droplets entrapped in the adhesive, compared to mild air-blowing techniques [165,191]. So, the clinician must increase the air-blowing time but should note the components of the adhesive in use.
Use of Matrix Metalloproteinase Inhibitors
Incomplete penetration of the resin into the demineralized dentinal matrix results in exposed, water-filled collagen fibrils that remain unprotected against denaturation. These collagen fibrils are susceptible to cleavage by both endogenous and exogenous collagenolytic enzymes [192]. Host collagenolytic enzymes, such as MMPs and cysteine cathepsins, collectively referred to as ‘dentin degradomics’, play a crucial role in resin-dentin bond failure, both during and after dentin demineralization. Research in this field is being developed to suggest new directions on the way of preventing their activity [193,194]. Adhesive layers fail because of the formation of micro-gaps infiltrated by pathogens [195]. Some of the different strategies proposed to minimize degradation include the deactivation of endogenous enzymes by using MMP inhibitors [196], the reinforcement of collagen fibrils within resin-dentin HL by using crosslinking agents and/or a combination of both strategies [194,197-199]. Apart from MMPs, the HL may be affected by a group of enzymes, namely cysteine cathepsins, which are endopeptidases produced by various cell types, including odontoblasts and pulp tissue cells [77]. Cysteine cathepsins hydrolyze the extracellular matrix, particularly in the collagen, and, like MMPs, they appear to be involved in the degradation of the exposed collagen at the bottom of the HL [56].
Several findings have suggested the use of protease inhibitors to enhance the longevity of resin-dentin bonds [126,200]. CHX, a broadly used antimicrobial agent, binds electrostatically to anionic sites of mineralized dentin, preserving resin-dentin bonds for up to 12 weeks [201]. It effectively inhibits MMPs and some CHX ions are retained within the HL even after 10 years of accelerated aging, although its mild transdentinal toxicity limits its application [202,203]. Epigallocatechin-3-gallate, including a green tea polyphenol [204], inhibits MMP-2 and MMP-9, improving resin-dentin durability [197]. Other agents like galardin [125], tetracyclines [205], quaternary ammonium salts and Ethylenediaminetetraacetic Acid (EDTA) have shown potential in inhibiting MMPs and enhancing bond stability [206,207]. Commercial products, such as etching gels with benzalkonium chloride [208] and adhesives with incorporated CHX also demonstrate anti-MMP effects, though their long-term efficacy varies [209].
Use of Crosslinking Agents
For years, numerous attempts have been made to achieve reliable and predictable adhesion of composite resin to tooth structure, as a strong bond ensures high retention strength, reduced microleakage and long-lasting restoration stability [210]. Long-term adhesion is directly linked to the stability and integrity of collagen fibrils within the resin-dentin HL [194]. In restorative dentistry, the mechanical properties of collagen are crucial [193]. The resin-tooth interface should exhibit minimal biodegradation to guarantee the longevity of the restoration [211]. Enhancing the mechanical stability and physico-mechanical properties of collagen can be achieved through various biomodifications, including the use of collagen crosslinking agents. Pre-treatment of the dentin surface with these agents prior to bonding procedures may improve BS values and increase the stiffness of the resin-dentin bond [193,194]. The covalent crosslinks formed by external crosslinking agents can be highly stable over time, deactivating the active sites of dentin proteases, reducing molecular mobility and inducing conformational changes in their structure. This results in a shift from negatively charged, ionized carboxyl groups to positively charged amides, thereby strengthening the collagen fibrils in the HL through intermolecular crosslinking [212]. Various natural and synthetic crosslinking agents offer significant advantages in developing mechanically stable collagen scaffolds [213]. For instance, Glutaraldehyde enhances dentin collagen properties but is hindered by its toxicity [214], while carbodiimides like Ethyl-3-[3-dimethylaminopropyl] Carbodiimide Hydrochloride (EDC) provide biocompatibility and improve mechanical properties without residual chemicals [215]. Naturally derived crosslinkers, such as proanthocyanidins, tannic acid, hesperidin, genipin, riboflavin and ribose, also show promising results by enhancing BS and stability, inhibiting enzymatic degradation and maintaining mechanical properties, albeit with varying mechanisms and potential drawbacks [194,213-217].
Crosslinking agents can improve the stiffness and stability of the HL by strengthening the collagen network, enhancing bonding to the dentin surface. However, while the increased stiffness can enhance durability and resistance to degradation, it may also reduce the mechanical flexibility of the HL. This reduction in flexibility could make the layer more brittle under mechanical stress, leading to potential failure of the bond during function. Therefore, the application of crosslinkers requires careful consideration of the balance between stiffness and flexibility [218].
Electric Current
An adhesive application protocol that incorporates the use of an electric signal has been introduced by some investigators [219-221]. The use of Ultrasonic (ULA) electric signals has proven to be an effective modification of standard clinical protocols, demonstrating improvements in bonding performance. Many studies demonstrated that ULA improves the dentin BS of both ER and SE adhesives when using an ULA vibrational energy [222,223].
Additionally, it was previously proven that an application assisted by an electric current and the Active Application (AA) of bonding agents improved the dentinal bond performance of the etching mode by easing the diffusion of adhesive monomers to the dentinal tubules [23]. Additionally, the application of an adhesive using an electric current enhances the chemical interaction between resin monomers and the dental substrate. This process increases monomer infiltration into the demineralized dentin by altering the surface charges and hydrogen bonding potential of the dentin, thereby improving BS. On that account, dentinal wettability increases, allowing the solvent to evaporate [224,225].
The use of an electric current could enhance resin monomer diffusion into etched dentin, as polar components such as HEMA, polyalkanoic acid, biphenyl dimethacrylate copolymers and PENTA present in the adhesive formulation may interact with the electric field [226]. Previous studies suggest that electrical currents can promote the mobility of ionized substrates. However, it remains unclear whether this process effectively generates proper dentin hybridization by facilitating the impregnation of ionized substrates under different conditions while also improving water removal for SE adhesives [227,228]. Next, the application of an electric current may boost the water substitution rate by modifying water dipoles, hence favoring water-solvent exchange throughout resin infiltration [229]. It has been stated that the use of electric currents between 30 and 35 μA significantly increased the binding capacity and quality of the bond [230]. Bonding at 35 μA has been shown to be safe for cell viability [225]. Jang, et al., studied the effect of various agitation methods on adhesive layer formation of HEMA-free universal adhesive (G-Premio Bond (GC, Tokyo, Japan)) [231]. AA, Passive Application (PA) and ULA were compared as follows:
Ideally, the use of an electric current between 30 and 35 μA during the application of ER and SE adhesive systems has been claimed to increase the bonding of an adhesive to dentin by enhancing substrate impregnation [232].
Field Control
An optimal use of rubber dam isolation (Fig. 7) prevented contamination of the prepared tooth from saliva, hemostatic agents, and/or blood and enhanced bond durability [233].

Figure 7: The importance of rubber dam isolation in bonding procedure (courtesy of Prof. Louis Hardan).
Saliva constitutes more than 99% of water and hence causes an excess of moisture, which ultimately lowers the BS [234,235]. It was found that dental substrates contaminated with an organic film of saliva generate a very low surface tension and hinder the wetting of the adhesive, resulting in a lack of good bonding [236]. In addition, saliva contains hydrolytic enzymes such as amylase, collagenase, esterase and ptyaline, all of which are capable of degrading collagen fibers and proteins, potentially jeopardizing the fundamental stability of the HL due to the formation of a thick smear layer or collagen fiber depletion [234,235,237].
A prior study found that contamination following etching had a negative influence on adhesion; however, blotting and applying a chemical primer may restore the BS [238]. Furthermore, it has been suggested that dentin contamination with saliva following etching reduces dentin bonding by 40% and that re-etching is required to improve the BS [239]. Drying without rinsing after saliva contamination may not be effective in eliminating some organic components and salivary glycoproteins because it hinders the resin composite from interacting with the oxygen inhibition layer [240]. In consequence, rinsing is mandatory when the dentin is contaminated with saliva. This is consistent with previous results that found no difference between the non-contaminated (control) and saliva-contaminated groups that were rinsed afterwards [241,242].
Moreover, if contamination occurs after primer application, the primer’s hydrophilic properties repel water from saliva, leading to a reduced degree of conversion [243]. Additionally, it has been noted that saliva contamination between etching and bonding, without rubbing the adhesive, could impact the bonding effectiveness to dentin. Therefore, rubbing the adhesive may enhance dentin BS in the presence of saliva [240]. Furthermore, in cases of salivary contamination occurring after adhesive polymerization, water decontamination should be performed, followed by reapplication of the adhesive [244].
Kim, et al., studied the effect of saliva decontamination procedures on dentin BS after curing of a universal bonding agent [242]. All-Bond Universal (Bisco, Inc., Schaumburg, Illinois, USA) was used in this study and then subjected to salivary contamination after curing. The authors proposed simply rinsing and drying to restore the Shear Bond Strength (SBS) to dentin, while re-etching and additional adhesive application proved to be effective in improving the BS.
In summary, (1) rinsing, drying and rebonding; (2) rinsing, air-drying and rebonding; (3) etching, rinsing, blot-drying and rebonding; or (4) etching, rinsing and drying might be adequate for reducing the unfavorable influence of saliva [237]. Blood is made up of macromolecules, proteins and platelets, which form a layer on the dentin surface due to dentin’s affinity for proteins, hindering resin penetration and resulting in shallower RTs development [237]. This was demonstrated by Hoorizad, et al., who found that blood or salivary contamination decreases resin-dentin BS in both SE and ER strategies [245].
Incomplete removal of blood proteins, residual water or decreased surface tension post-washing can lead to reduced wetting ability of the resin composite surface for subsequent layers [237]. However, rinsing the contaminant substance, particularly blood, in an attempt to boost dentinal BS, failed to restore non-contaminated values [246,247]. Finally, when blood contamination occurs, it is supposed that rinsing and applying an adhesive system improves adhesion to the subsequent composite layer. Moreover, using 5.25% sodium hypochlorite for less than 60 s effectively counteracted the contamination impact, owing to its nonspecific proteolytic ability to remove organic remnants without negatively affecting adhesion [243,248]. Moreover, re-etching facilitates adhesion by altering organic residues, reducing their affinity to the substrate underneath, thus making it an appropriate step for rinsing [249].An alternative option recommended to counteract the adverse impact of blood contamination on dentin BS involves the use of hemostatic agents as preventive measures. Hemostatic agents such as aluminum chloride, ferric sulfate and tannic acid are commonly employed to stop bleeding. However, some of these chemicals can reduce the BS of dental adhesives [250]. Typically, these agents are applied around the gingiva, where bleeding is prevalent. Prior studies have demonstrated that aluminum chloride and ferric sulfate dentin contamination can significantly reduce the BS of SE adhesive when compared to normal dentin (uncontaminated) [251,252]. This was related to the agents’ proprietary fumed silica, which may have inhibited their acidic activity. Moreover, clinicians should use caution when employing these compounds in esthetic restorations due to the potential for discoloration combined with a reduction in BS [237].
Concerning the use of hemostatic agents in a clinical setting, it is noteworthy that bleeding may appear during various stages of both direct and indirect restoration procedures, such as preparation, gingival retraction and luting, particularly in cases where a subgingival margin is involved [253,254]. In such scenarios, dental practitioners often apply the hemostatic agent to all surfaces of the teeth, leading to significant surface exposure to the agent rather than blood contamination [255]. However, due to the detrimental effect of hemostatic agents on the BS of resin-based materials, their application is not recommended in cases of blood contamination. Some experts recommend applying EDTA or CHX in order to reestablish the BS between dentin and a resin composite in cases of accidental surface contamination with a hemostatic substance [251,256].
All in all, to restore the quality of the bond after contamination, decontamination methods can include rinsing and drying followed by the reapplication of the adhesive, drying the contaminants before reapplying the adhesive or performing re-etching and re-bonding [257].
Selective Dentin Etching
UAs have garnered significant research interest in recent years due to their versatility in being used in SE, ER and selective-etching modes. Notably, the ability to utilize this new class of adhesives, regardless of the dentin condition, opens up new possibilities for resin-dentin bonding to selectively etched substrates [258]. Van Meerbeek, et al., suggested that protecting collagen from hydrolysis and early degradation of the bond could be achieved by maintaining HAp around the collagen fibrils [259]. Recently, a new approach known as “Selective Dentin Etching” (SDE) was orchestrated to improve bonding to dentin by preserving HAp crystals inside the hard-to-reach intrafibrillar collagen spaces [260] (Fig. 8).

Figure 8: Selective dentin etching involves the application of phosphoric acid for 3 s on dentin, followed by rinsing and drying, resulting in a partially demineralized substrate (courtesy of Dr. Rim Bourgi). This technique differs from etch-and-rinse, where both enamel and dentin are etched, rinsed and bonded; Selective enamel etching: where etching is performed only on enamel; Self-etch, where no phosphoric acid is applied to either enamel or dentin, as the bonding agent etches and bonds simultaneously.
This technique involves the application of H3PO4 for 3 s on dentin, followed by rinsing and drying, resulting in a partially demineralized substrate. This method has been recognized as an alternative for increasing the BS of UAs to dentin over time [258]. In 2016, Takamizawa, et al., determined the effect on dentin bonding of H3PO4 pre-etching times before the application of SE adhesives [261]. They concluded that reducing H3PO4 pre-etching time can diminish the adverse influence on dentin bonding durability for the conventional SE adhesives. Also, a short H3PO4 pre-etching time enhances the dentin bonding performance of UAs. In 2018, Stape, et al., evaluated whether SDE protocols using reduced H3PO4 etching times would affect the resin-dentin interaction of a universal bonding agent to improve long-term bonding effectiveness [258]. They advised that UAs used in SE mode produce superior long-term dentin bonding compared to the ER mode and SDE for 3 s with conventionally used H3PO4 improves dentin bonding effectiveness.
In 2019, Kharouf, et al., evaluated the effect of etching with the rubbing technique on the BS of a universal bonding agent to dentin [262]. They demonstrated that dentin etched with H3PO4 for 3 s in the ER mode with the rubbing technique for a universal adhesive system decreases the μTBS of the composite to dentin. Additionally, they confirmed that SDE with 37% H3PO4 for 3 s without rubbing motion before applying a universal adhesive is recommended to enhance bonding effectiveness (Fig. 9).

Figure 9: Scanning electron microscope image of the dentin-adhesive interface in bonded dentin using a universal adhesive in the etch-and-rinse mode without the rubbing technique, showing the uniform and complete filling of dentinal tubules (×1200 magnification) (courtesy of Prof. Naji Kharouf).
In 2021, Stape et al., evaluated whether the bonding performance and fatigue strength of resin-dentin interfaces created by a universal adhesive were affected by different H₃PO₄ application times, in order to more accurately assess long-term durability [263]. They found that removing the smear layer with H3PO4 significantly improved the endurance limits of bonded interfaces, particularly for shorter dentin-etching times. Conventional H₃PO₄ dentin etching enhances fatigue strength; however, overexposing collagen fibrils can lead to endogenous proteolytic hydrolysis over time, ultimately diminishing these benefits.
In 2021, Hardan, et al., assessed the influence of AA for different time intervals after SDE for 3 s on the μTBS to dentin of two UAs [260]. They discovered that SDE and AA improved the μTBS only for a HEMA-containing universal bonding agent.
In 2022, Stape, et al., determined whether smear layer management, through conservative etching protocols and the hydrophobic-rich content of the HL would impact the fatigue strength of resin-dentin interfaces [264]. They suggested that current trends in simplifying resin-dentin bonding involve a trade-off between hybridization quality and improved adhesive handling. To extend the longevity of mild UAs, controlled dentin etching and an increased hydrophobic content in the HL could be crucial.
In 2024, Stape, et al., investigated the effects of extending dentin etching and the hydrophobic-rich content of hybrid layers on the fatigue strength of a mild universal adhesive after long-term aging [265]. They observed that long-term hydrolysis has a detrimental effect on the fatigue strength of resin-dentin interfaces. The study emphasized the importance of employing less aggressive ER protocols and developing hybrid layers with higher hydrophobic content to improve the durability of mild UAs. Consequently, current trends toward oversimplification in adhesive dentistry may compromise resin-dentin bonding performance.
In spite of this, the authors of a former review believe that the allocated term “SDE” may confuse researchers. They propose short dentin etching as a more appropriate name for etching times of less than 15 s [266]. This approach could minimize the risk of unintentional dentin etching while preserving most of the minerals necessary for successful adhesion. However, applying the etchant for such a brief period may be clinically challenging. Further research is needed to develop an etching technique that balances clinical requirements with the preservation of HAp.
Due to the heterogeneity of the dental substrate, which makes H3PO4 etching highly unpredictable, it would be beneficial to have a “universal etchant” capable of effectively etching enamel and dentin concurrently. Such a material might be advantageous in difficult clinical situations such as deep posterior proximal cavities, where assessing leftover enamel and ensuring optimal bonding conditions can be problematic [260,266,267].
So, after showing the literature assessing the use of SDE for 3 s on dentin substrate, clinicians could choose this approach in their daily clinical practice by taking into consideration the viscosity of the etchant. A new protocol, SDE for 3 s with the ER technique, is recommended before applying the UAs on the dentin surface in order to improve BS [258,261].
Enhanced Dentin Impregnation Using a Scrubbing Technique
Increasing the application time of adhesive systems with a vigorous brushing method has the potential to boost dentin impregnation of resin monomers into dentinal tubules [57,187]. Hardan, et al., advocated the use of scrubbing motion when bonding to dentin to improve the immediate and aged BS [23]. Moritake, et al., studied the effect of AA on the bond durability of three UAs (All-Bond Universal (Bisco, Inc., Schaumburg, IL, USA), Adhese Universal (Ivoclar Vivadent, Schaan, Liechtenstein) and Scotchbond Universal (3M ESPE, St. Paul, MN, USA)) [268].
Moritake, et al., concluded that the AA of UAs enhanced dentin bond durability of the etching mode by facilitating the penetration of adhesives into the branches of dentin tubules [268]. Additionally, Carrilho, et al., proposed an adhesive application technique involving scrubbing, which enhances the impregnation of monomers into the smear layer, facilitates solvent evaporation and thereby enhances the quality of the adhesive interface [269]. The same finding was observed by Velasques, et al., who showed that AA of SE adhesive could enhance bonding as a mechanism similar to that of ER bonding agents by increasing the interaction of acidic monomers with the tooth structure and dispersing etching byproducts through the HL [270]. Velasques, et al., brought attention to the fact that modifying the application time of the adhesive could influence BS [270]. Furthermore, Irmak, et al., proposed that the rubbing action elucidates the process, revealing that it decreases the degradation rate of the HL by facilitating the diffusion of resin monomers into the collagen fibrils [271]. This highlights why manufacturers of certain adhesives advocate for an AA method [272]. Aside from that, after manually applying force through a rubbing motion with adhesive onto the dentinal tissue, dentin exhibits characteristics similar to a sponge, with the dentin collagen network being compressed. Compressed collagen expands when pressure is relieved and the penetration of resin monomers into the collagen network is promoted. This method does not require any additional steps [23,272] (Fig. 10).

Figure 10: An example of active bonding application of a universal adhesive system on a dentinal surface, showing clear lateral connections. The scanning electron micrograph highlights distinct structural integrity across the bonded interface (courtesy of Dr. Rim Bourgi).
Biomimetic Remineralization
In 2008, Tay and Pashley introduced a guided tissue-remineralization technique to repair HL and prevent degradation within adhesive-dentin interfaces [273]. However, its applicability in vivo remains unclear [57,274]. In response, Daoud U and Fawzy A, proposed High-Intensity Focused Ultrasound (HIFU) for dentin-substrate biomodification, showing potential for improving remineralization [275]. They suggest HIFU as a minimally invasive technique capable of delivering HAp nanorods into etched dentin substrates, enhancing remineralization.
Biomimetic remineralization is an emerging area of research showing promise in the treatment of dentinal lesions. While laboratory-based studies have demonstrated significant efficacy, clinical trials and in-vivo studies are still in early stages. In a systematic review that assessed various biomimetic agents, it was found that these agents, particularly non-collagenous protein analogs and bioactive materials, achieved substantial remineralization, improving the mechanical properties of dentin to near-natural levels [276].
However, most of these studies were conducted under controlled in-vitro conditions, which may not fully replicate the complexities of the natural oral environment. Though there is growing evidence supporting the efficacy of biomimetic remineralization, additional long-term clinical trials are needed to assess the full potential and reliability of these techniques in real-world, in-vivo settings.
Dentin Pre-Treatment with Airborne Particle Abrasion
In modern adhesive dentistry, Airborne Particle Abrasion (APA) is commonly recommended to finish cavity preparation for adhesive restorations. APA has become more convenient with devices that combine abrasive particles and water to control their dispersion [277]. Aluminum Oxide (AO) powder, available in 30 and 50 µm sizes, is frequently used for this purpose. It enhances surface roughness and wetting ability, aiding in micro-mechanical retention [278]. While a prior study generally shows no adverse effect on enamel BS, evidence regarding its impact on dentin BS is conflicting [277]. Positive effects on dentin bonding have been reported while others suggest a decrease in BS [280], especially with SE adhesives [279]. However, indications from research suggest that AO air-abrasion is safe for dentin bonding, with no impairment noted [279].
In addition to AO powders, there are fewer abrasive powders used to clean cavity preparations and remove biofilm, plaque or stains before restoring teeth with adhesive materials. These include sodium bicarbonate, calcium carbonate, aluminum trihydroxide, bioactive glass, glycine and erythritol [278,281,282]. It was demonstrated that sodium bicarbonate air polishing can lead to decreased dentin BS, particularly with SE adhesives. Similar effects were observed with calcium bicarbonate and erythritol in combination with different adhesives. However, air polishing with bioactive glass and glycine did not have a negative impact on dentin BS. The significant variation in dentin bonding effectiveness across different in-vitro studies can be attributed to the wide variety in study designs [278].
Numerous parameters impact the cutting efficiency of airborne abrasion devices, including pressure, duration of air-abrasion or polishing, distance, angle towards the dentin surface, type of dentin, nozzle diameter, powder flow rate, water shrouding flow rate, type of powder and particle size. These parameters vary significantly between studies and some studies do not even specify certain parameters. Moreover, the type of BS test conducted influences the final result [278,282]. Currently, there is limited literature available that evaluates the effect of air-abrasion or polishing on dentin BS over time.
A preceding study investigated how APA affects the strength of bonds between adhesive materials (universal adhesive) and dentin, using different air-abrasion and polishing powders. The results showed that when using a universal adhesive, applying it with the ER mode is better than the SE mode for bonding to air-abraded or polished dentin.
In summary, the effectiveness of air-abrasion in bonding to dentin can vary depending on various factors such as the type of adhesive used, the specific parameters of the air-abrasion procedure and the type of dentin being treated. While some studies suggest that air-abrasion can enhance micro-mechanical retention and improve BS to dentin, others report conflicting results. Overall, air-abrasion may be effective in certain situations and when used with appropriate techniques, but further research is needed to fully understand its impact on dentin bonding [278,281-283].
Use of Dimethyl Sulfoxide (DMSO)
Dimethyl Sulfoxide (DMSO) is a polar aprotic solvent known for its ability to penetrate biological tissues and modify collagen structures. Recent studies have explored its potential to enhance resin-dentin bonding by improving adhesive monomer infiltration and HL quality. DMSO facilitates the disruption of water-collagen interactions, increasing the interfibrillar spacing within the dentin matrix and promoting deeper monomer penetration into collagen fibrils [284,285].
Additionally, DMSO may enhance the durability of the adhesive interface by reducing the enzymatic activity responsible for collagen degradation. Salim Al-Ani, et al., demonstrated that different DMSO concentrations can significantly improve long-term BS and HL integrity when applied prior to the bonding procedure [286]. Zhang, et al., further supported these findings in their systematic review, highlighting the promising role of DMSO in optimizing resin-dentin adhesion and minimizing NL over time [284].
These findings suggest that the incorporation of DMSO as a dentin pre-treatment could represent a valuable addition to clinical protocols aimed at improving the longevity of adhesive restorations. However, further research is needed to establish standardized application protocols and assess its biocompatibility in long-term clinical settings (Table 1).
Application Modality | Description | Effect on Bond Strength (BS) |
Hydrophobic Resin Layer [111,120,122] | Adding a final hydrophobic resin layer to seal the adhesive interface. | Reduces water sorption and resin degradation, improving BS. |
Double Adhesive Application Time [22,23] | Prolonging the adhesive dwell time on dentin. | Ensures optimal monomer penetration and polymerization, enhancing BS. |
NTAP (Non-Thermal Atmospheric Plasma) [134,135] | Using plasma to clean and activate the dentin surface. | Increases surface energy and wettability, improving adhesive infiltration. |
Ethanol Wet-Bonding (EWB) [144,145] | Keeping the dentin surface wet with ethanol instead of water during adhesive application. | Reduces collagen collapse, ensuring deeper adhesive penetration. |
Acetone Wet-Bonding (AWB) [149,150] | Similar to EWB but uses acetone to keep dentin moist. | Enhances primer penetration into demineralized dentin. |
Multiple Coats of Adhesive [22,23,151] | Applying two or more layers of adhesive resin. | Improves hybrid layer uniformity and adhesive strength. |
Warm Air Stream on Primer or Adhesive [19,167,168] | Applying warm air to evaporate residual solvents before light curing. | Prevents solvent entrapment, increasing hybrid layer quality. |
Prolonged Curing Time [22,23] | Extending light curing time to up to 40 s. | Ensures complete polymerization, increasing mechanical properties. |
Prolonged Air-Drying [22,23] | Drying adhesive for an extended time before curing. | Improves solvent evaporation and adhesive layer consistency. |
MMP Inhibitors [205-209] | Application of agents like chlorhexidine to inhibit matrix metalloproteinases. | Reduces collagen degradation at the adhesive-dentin interface. |
Crosslinking Agents [193] | Using agents to crosslink dentin collagen. | Enhances collagen stability and hybrid layer durability. |
Electric Current-Assisted Application [23] | Using mild electric currents to enhance adhesive penetration. | Increases resin infiltration and BS. |
Strict Isolation Techniques [81,283] | Ensuring a dry field using rubber dams or isolation devices. | Prevents contamination, ensuring better adhesive interaction. |
Short-Duration Etching (SDE) [258,260] | Reducing etching time to 3 s. | Prevents over-etching, preserving hydroxyapatite crystals inside the hard-to-reach intrafibrillar collagen spaces. |
Scrubbing Technique [272] | Actively scrubbing adhesive onto dentin. | Increases mechanical interaction and resin infiltration. |
Biomimetic Remineralization [275,276] | Using bioactive materials to remineralize dentin before bonding. | Enhances mineralization and BS durability. |
Air-Particle Abrasion (APA) [278,281,282] | Sandblasting the surface with fine particles. | Cleans and roughens the surface, improving mechanical adhesion. |
Dimethyl Sulfoxide [284-286] | Use of Dimethyl Sulfoxide solution to etched dentin with a microbrush | Enhances resin-dentin adhesion |
Table 1: Summary of adhesive application modalities used in this research that enhance resin-dentin bond strength through various techniques and modifications to the manufacturer’s recommendations, highlighting their effects on hybrid layer formation and durability.
Limitations
This review is limited in several key areas. It focuses primarily on bonding to sound dentin, leaving the behavior and challenges of pathological dentin, such as sclerotic or carious substrates, underexplored. Furthermore, factors like simulated pulpal pressure-critical for mimicking in-vivo conditions-were not consistently accounted for in the reviewed studies. Bonding to enamel, another crucial substrate in adhesive dentistry, was not comprehensively addressed. Additionally, variations in smear layer characteristics and the lack of standardization in its preparation across studies introduce potential inconsistencies. The influence of cavity type and configuration on bonding performance and its implications in clinical settings were also not thoroughly analyzed. Finally, the findings largely focus on direct restorations, overlooking the specific bonding requirements and challenges associated with indirect restorations.
Discussion for Future Directions
Future research should explore adhesive performance under simulated pulpal pressure to replicate in-vivo conditions more accurately. Investigations into bonding to pathological or deep dentin including sclerotic, carious and eroded substrates, are necessary to address real-world clinical scenarios [287]. The development of standardized protocols for smear layer preparation and its characterization would enhance comparability across studies. Additionally, analyses should investigate the interaction of adhesives with enamel substrates and their performance in various cavity configurations. Research into adhesive bonding for indirect restorations is paving the way for innovations that enhance clinical efficiency and outcomes [288]. A promising development is the recently introduced self-cured bulk-fill resin-based composite, Stela (SDI, Bayswater, Victoria, Australia), designed as a high-performance “amalgam alternative” [289]. This material eliminates the need for a light-curing unit, allowing unlimited depth of cure while maintaining superior aesthetics compared to traditional amalgam restorations. The Stela system integrates a novel primer free of tertiary amines, featuring Glycerol-Dimethacrylate (GDMA), which enhances polymerization, mechanical properties and adhesion to dentin while reducing water uptake and solubility. Stela Automix, combined with its self-curing adhesive system, leverages advanced fillers such as strontium fluoroaluminosilicate, ytterbium trifluoride and calcium aluminate to ensure robust mechanical strength and biocompatibility. The composite polymerizes upon contact with the primer, streamlining the bonding process and creating a secure tooth-restorative interface [290].
By integrating the unique primer formulation and advanced filler technology, Stela represents a significant step toward the future of adhesive dentistry. This innovation underscores the potential for developing materials that combine simplicity, efficiency and enhanced clinical performance, aligning with the evolving demands of restorative dental practices.
Conclusion
This review highlights several strategies that have been shown to enhance adhesive BS to dentin, emphasizing that a standardized protocol for achieving optimal adhesion is still lacking. Among the effective techniques discussed are the use of a hydrophobic resin layer, an extended adhesive application time, NTAP, EWB and AWB, multiple adhesive layers (two or more), a warm air stream (50-60°C) on the primer or adhesive system and an extended curing time (up to 40 s). Prolonged air-drying, the prior application of MMP inhibitors, crosslinking agents and electric current-assisted application, along with an appropriate isolation using a rubber dam, SDE for 3 s, the scrubbing technique, biomimetic remineralization, an APA for dentin pre-treatment and the use of DMSO were also found to improve BS. These strategies, when applied correctly, have the potential to significantly enhance adhesive performance and increase long-term durability. Notably, no single method was found to be entirely superior; instead, a combination of these strategies can lead to optimized BS. Despite the lack of a universally accepted protocol, the findings suggest that achieving durable resin-dentin bonds require a tailored approach, a thorough understanding of adhesive chemistry and clinical innovation. The reviewed strategies are crucial for improving the longevity and reliability of dentin restorations and clinicians must carefully select and apply these techniques to maximize adhesive performance and ensure the success of restorative treatments.
Conflict of Interest Statement
All authors declare that there are no conflicts of interest.
Informed Consent Statement
Not applicable.
Authors’ Contributions
Conceptualization, R.B. and L.H.; methodology, R.B.; software, R.B. and N.K.; validation, Y.H., C.E.C.-S., N.N. and R.B.; formal analysis, L.H.; investigation, R.B., N.N., Y.H., N.K. and L.H.; resources, R.B.; data curation, R.B.; writing-original draft preparation, R.B.; writing-review and editing, Y.H., C.E.C.-S., N.K. and L.H.; visualization, R.B. and L.H.; supervision, L.H., Y.H. and N.K.; project administration, R.B., L.H., Y.H. and N.K.; funding acquisition, R.B. All authors have read and agreed to the published version of the manuscript.
Financial Disclosure
The authors received no external financial support for this study.
Ethical Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Reference
