Research Article | Vol. 7, Issue 1 | Journal of Ophthalmology and Advance Research | Open Access |
Yinon Shapira1,2*![]() , Valerie Juniat3, Tarjani Dave4, Stephen Santoreneos5, Jeffrey A Nerad6, Dinesh Selva7
, Valerie Juniat3, Tarjani Dave4, Stephen Santoreneos5, Jeffrey A Nerad6, Dinesh Selva7
1Department of Ophthalmology, Carmel Medical Center, Haifa, Israel
2The Bruce and Ruth Rappaport Faculty of Medicine, Technion-Israel Institute of Technology, Haifa, Israel
3Department of Ophthalmology, Sussex Eye Hospital, Brighton, UK
4Ophthalmic Plastic Surgery Service, L V Prasad Eye Institute, KAR Campus, Hyderabad, Telangana, India
5Department of Neurosurgery, Royal Adelaide Hospital, Adelaide, South Australia, Australia
6Cincinnati Eye Institute, Cincinnati, Ohio, USA
7Department of Ophthalmology, Royal Adelaide Hospital and South Australian Institute of Ophthalmology, Adelaide, South Australia, Australia
*Correspondence author: Yinon Shapira, Department of Ophthalmology, Carmel Medical Center, Haifa, Israel; Email: [email protected]
Citation: Shapira Y, et al. Orbito-Cranial Cavernous Venous Malformation: A Case Series and Review of the Literature. J Ophthalmol Adv Res. 2026;7(1):1-10.
Copyright: © 2026 The Authors. Published by Athenaeum Scientific Publishers.
This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
License URL: https://creativecommons.org/licenses/by/4.0/
| Received 06 March, 2025 | Accepted 30 March, 2026 | Published 06 April, 2026 |
Purpose: To describe the features, surgical approaches and outcomes of orbito-cranial Cavernous Venous Malformation (CVM).
Study Design: Multicenter retrospective case-series and review of the literature
Methods: Patients with CVM managed in three orbital services over six years were identified. Data collected included demographics, presenting features, neuroimaging, histology, surgical approach, complications and outcomes.
Results: Three female patients, aged 52, 59 and 68 years, with CVM were included. All had gradually decreasing visual acuity and signs of optic neuropathy. One had slowly progressive proptosis. CT or MRI revealed well-circumscribed, intraconal masses involving the deep orbital apex and superior orbital fissure, with extension into the cavernous sinus in 2 cases. In the remaining case, the CVM involved almost the entire orbit with erosion through the roof. The two apical cases had complete excision via a cranio-orbital approach (stereotactic pteronial and fronto-orbitocraniotomy in one and an eyelid skin crease fronto-orbitocraniotomy in the other). Recovery of optic nerve function was noted postoperatively in both. Sequelae included pupil involving partial 3rd nerve palsy (resolved after six weeks) in the first case, persistent diplopia in the latter and hypoesthesia in both (improved over several months). The third case with extensive CVM underwent a transcaruncular biopsy due to diagnostic uncertainty. Uncontrollable massive intraoperative bleeding necessitated the conversion to eyelid sparing exenteration with subtotal tumor removal. No progression of the residual tumor was noted six months postoperatively.
Conclusion: These cases highlight the challenges of surgical excision in complex CVM. Meticulous preoperative neuroimaging to establish the diagnosis and a multidisciplinary approach are essential for successful management.
Keywords: Cavernous Venous Malformation; Cavernous Hemangioma; Orbital Apex; Intracranial; Superior Orbital Fissure; Complications; Radiotherapy
Orbital cavernous venous malformation (CVM), historically termed “cavernous hemangioma” or “cavernoma,” is now classified according to the International Society for the Study of Vascular Anomalies (ISSVA) as a low-flow venous malformation [1]. It is the most common benign orbital tumor in adults [2,3]. The most common location is the middle third of the orbit, in the intraconal space lateral to the optic nerve [4]. An orbito-cranial extension has been rarely reported, posing a challenge for surgical access [5-8]. We present three patients with orbito-cranial CVM, which were surgically managed and review the relevant literature.
This multicenter retrospective case series included adult patients with orbital Cavernous Venous Malformation (CVM) with orbito-cranial extension who underwent surgical treatment at three tertiary orbital referral centers: Cincinnati Eye Institute, Ohio, USA; L V Prasad Eye Institute, Hyderabad, India; and Royal Adelaide Hospital / South Australian Institute of Ophthalmology, Adelaide, Australia. Data were collected retrospectively from consecutive adult patients treated between 2017 and 2023. These cases represent all known orbito-cranial CVMs encountered at the participating centers during this period.
This study received approval from the Central Adelaide Local Health Network (CALHN) Human Research Ethics Committee (HREC) and CALHN Research Services (approval number 14862) and adhered to the tenets of the Declaration of Helsinki. Given the retrospective and anonymized nature of the study, the requirement for patient consent was waived by the ethics committee.
Included patients were adults (>18 years) with orbito-cranial CVM. Histopathological confirmation was obtained in all three cases and showed the typical features of cavernous venous malformation, namely large dilated vascular spaces lined by flattened endothelial cells, separated by fibrous septa and enclosed by a fibrous pseudocapsule [9]. Data collected included patient demographics, presenting symptoms and signs, duration of symptoms, neuroimaging characteristics of the tumor, histology, management course, treatment-related complications, length of follow-up and clinical status at the final follow-up. All cases were reviewed in a multidisciplinary setting with neuroradiological input.
A targeted narrative literature review was also performed to identify previously reported cases of orbito-cranial cavernous venous malformation. PubMed was searched using combinations of the terms “orbital cavernous venous malformation”, “orbital cavernous hemangioma”, “orbital cavernoma”, “intracranial”, “cavernous sinus”, “orbital apex”, “superior orbital fissure”, “craniotomy”, “cranio-orbital” and “transorbital”. Additional relevant articles were identified through review of reference lists. Only English-language reports were included.
Case 1
A 59-year-old female presented with gradually deteriorating left vision over four years. Her ophthalmologist had documented a progressive left Humphrey Visual Field (VF) superior arcuate defect over the same period. Her distance corrected visual acuity (DCVA) was 6/7.5 right and 6/9 left, with a left Relative Afferent Pupillary Defect (RAPD). She did not have optic disc pallor or edema, proptosis or extraocular motility limitation. Magnetic Resonance Imaging (MRI) demonstrated an enhancing, well-circumscribed 11mm lesion at the left orbital apex, displacing the optic nerve medially (Fig. 1). The lesion extended to the Superior Orbital Fissure (SOF) without clear evidence of Cavernous Sinus (CS) involvement. The patchy enhancement pattern prompted a working diagnosis of CVM or, less likely, a schwannoma. She was referred to a neuro-oncology Multidisciplinary Team (MDT), where it was decided that excision was feasible and preferable to radiotherapy.
The patient underwent a joint neuro-orbital stereotactic left pteronial and orbitofrontal craniotomy. An extradural clinoidectomy with decompression of the optic foramen and a lateral wall (extradural) approach to the CS were performed. Intraoperatively, a vascular lesion extended from the orbital apex through the SOF to the anterior CS. The lesion was adherent to the 3rd and 4th cranial nerves and was completely excised. Histopathology confirmed CVM.
Postoperatively her visual acuity was unchanged and she had a partial pupil involving 3rd nerve palsy with mild ptosis, which resolved over six weeks. Temporal hypoesthesia persisted at four-month follow-up but improved at six months. Visual fields at four months indicated a recovery of optic nerve function. Her MRI (Fig. 1) 15 months postoperatively indicated no recurrence.
Case 2
A 52-year-old female had a 6-year history of painless, slowly progressive proptosis and deteriorating left vision. She had 7 mm of left axial proptosis, global limitation of extraocular motility, light perception (without projection) VA, optic atrophy and an RAPD. Computerized Tomography (CT) demonstrated an intraconal, well-circumscribed, homogenous, 41mm lesion (Fig. 2). It occupied almost the entire anterior-posterior span of the orbit and all orbital quadrants. There was bony expansion of the medial orbital wall and widening of the SOF. Additionally, the orbital roof was eroded with tumor extension into the anterior cranial fossa (Fig. 2).
A differential diagnosis of CVM, schwannoma and solitary fibrous tumor was considered. The patient was advised to have further imaging with contrast; however, an exploratory biopsy was undertaken next due to socio-economic reasons and resource unavailability. A trans-caruncular approach revealed a whitish, soft encapsulated lesion that did not have the typical appearance of a CVM. An incisional biopsy was sent for frozen section, resulting in torrential bleeding at multiple sites within the lesion. Attempts to achieve hemostasis (i.e., pressure, electrocautery, hypotensive anesthesia, reverse Trendelenburg, intravenous ethamsylate, application of cyanoacrylate glue and tranexamic acid-soaked gelfoam) continued for one and a half hours but failed to control the active bleeding. An estimated blood loss of 350cc was recorded. After discussion with the patient’s family, it was decided to proceed with an eyelid sparing exenteration. The orbital roof was dehiscent posteriorly; however, the dura was intact and no Cerebrospinal Fluid (CSF) leak occurred. The lesion was confirmed to be a CVM on histopathology. Separate samples sent from apical tissue confirmed residual tumor. Postoperatively there was no progression at six months of follow-up.
Case 3
A 68-year-old female had a 1-month history of intermittent diplopia, decreasing left visual acuity and minor left orbital pain and headache. She had a history of bilateral chronic angle-closure glaucoma with peripheral iridotomies. On examination, the DCVA was 6/7.5 in the right eye and 6/12 left, with a left RAPD. There was 1mm of left proptosis, with no limitation of extraocular motility. She had bilateral, symmetric glaucomatous optic disc cupping with inferior arcuate defects on Humphrey VF. CT and MRI revealed a 34mm, well-circumscribed, left orbital mass extending into the SOF (Fig. 3).
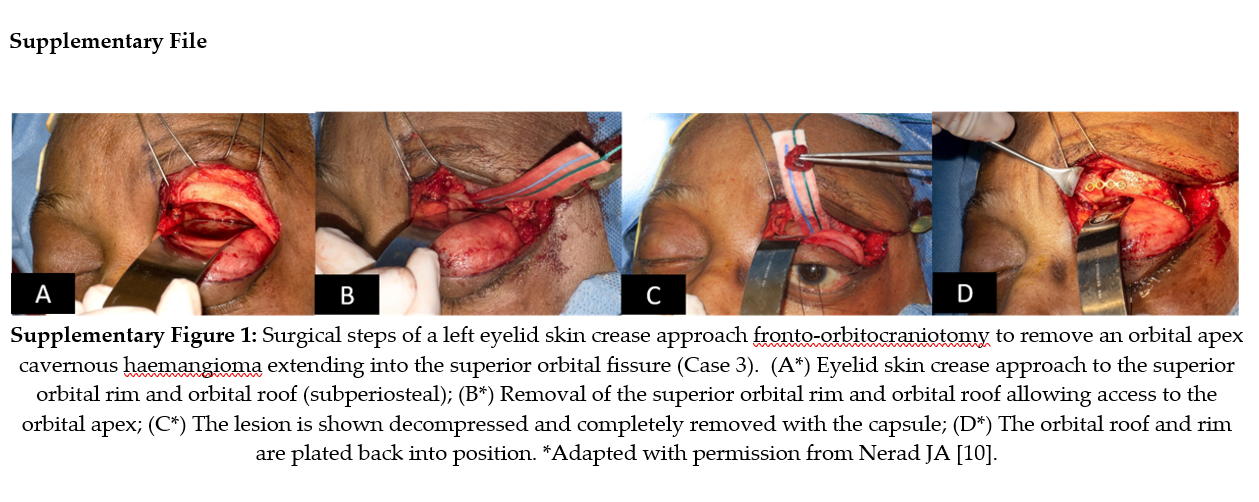
An eyelid skin crease fronto-orbitocraniotomy was conducted (Supplementary Fig. 1). The orbital rim and roof were removed, allowing access to the orbital apex and extradural mass exposure [10]. The operating microscope was used to provide illumination and magnification. The tumor was decompressed and completely removed (Supplementary Fig. 1). The orbital roof and rim were plated back into position following tumor excision. Histopathology confirmed CVM.
Postoperatively, VA was unchanged and the left RAPD had resolved. The patient developed a left ptosis and forehead hypoesthesia, both of which improved over 18 months without completely resolving. She also developed limited left upgaze and abduction with worsened diplopia. The motility objectively normalized over one year; however, the patient still experienced incomitant intermittent diplopia causing her to stop driving. There was no recurrence of the tumor 18 months postoperatively.

Figure 1: Pre- and postoperative MRI of Case 1. (A) T2-weighted fat-suppressed axial MRI showing an oval-shaped hyperintense lesion; (B) T1-weighted axial MRI showing an isointense lesion; (C) T1-weighted fat-suppressed post-contrast axial MRI showing an enhancing lesion at the left orbital apex abutting and displacing the ptic nerve medially. The lesion extends into the superior orbital fissure (arrow); (D) T1-weighted fat-suppressed post-contrast MRI at 15 months postoperatively showing no tumor recurrence.

Figure 2: Preoperative CT of Case 2. (A) Axial and (B) coronal non-contrast CT images (soft tissue windows) showing a diffuse homogeneous lesion extending from the left orbit into the anterior cranial fossa through superior bony wall erosion (black arrow), with associated medial wall expansion (white arrow).

Figure 3: Preoperative imaging of Case 3. (A*) Axial post-contrast CT and (B*) axial T1-weighted fat-suppressed post-contrast MRI showing a large enhancing intraconal mass extending into the superior orbital fissure (arrow). (C*) Coronal T2-weighted fat-suppressed MRI showing inferior displacement of the optic nerve (arrow). *Adapted with permission from Nerad JA [10].
Cavernous venous malformations epicentered in the orbit have rarely been reported to extend intracranially. Large lesions may extend into the cranial cavity via erosion of the orbital roof or apex. Small apical lesions may also extend through the superior orbital fissure or the optic canal. Only a limited number of case reports and small series describe this presentation and even fewer provide meaningful detail regarding surgical management and outcomes [5-8,11-14]. Previously reported cases are summarized in Table 3. The current series therefore adds one of the larger focused clinical experiences with this uncommon presentation. Thus, the management approaches and experience described herein from three orbital centers may benefit the orbital specialist encountering this infrequent presentation. Furthermore, the considerations discussed herein may apply to other deep apical lesions with intracranial extension where surgical resection risks significant collateral damage [15].
More than two decades ago, Mawn, et al., described two cases of apical CVM extending to the CS through the SOF, along with a third case of a deep apical CVM [5]. Both orbito-cranial cases had optic atrophy[5], while in the current series, it was encountered only in the case of the orbito-cranial CVM occupying the majority of the orbit. Of note, two of the orbito-cranial CVMs in the current series presented without or with only minimal proptosis, suggesting that compressive optic neuropathy may be the initial manifestation of these deep apical tumors. Mawn, et al., reported that one of the orbito-cranial cases and the apical CVM were totally excised via a fronto-orbital craniotomy [5]. Vision improvement was noted postoperatively. Nonetheless, they were complicated by CSF leaks, intraoperative in the former and postoperative (requiring repeat craniotomy) in the latter. In both patients, postoperative extraocular motility deficits resolved over time and a poorly reactive pupil remained in one.
Scheuerle, et al., previously reported high complication rates following a craniotomy approach for excision of apical CVMs [16]. Of 14 patients operated by frontotemporal craniotomy, three showed severe complications. One sustained a life-threatening subdural hematoma and permanent frontal lobe syndrome. Two other cases experienced severe, permanent postoperative decrease in vision. Temporary postoperative sequelae (usually resolving within a few weeks) were commonly observed in their series and included eyelid ptosis, extraocular motility impairment (with or without diplopia) and visual disturbances [16].
The third case described by Mawn, et al., was preoperatively suspected to be a schwannoma and it was thus approached via medial orbitotomy for biopsy [5]. The authors reported difficulty in exposing the lesion using this approach. Subsequently, the patient developed postoperative optic disc edema with vision loss and further developed meningitis. The diagnostic difficulty, biopsy approach and significant collateral damage are similar to case 2 in our series. Our case also highlights the possibility of massive bleeding during biopsy and/or surgical decompression of extensive orbital CVMs. This complication has previously only been rarely reported intraoperatively in more typical orbital CVM [17].
Although a number of orbital pathologies including schwannoma, meningioma, solitary fibrous tumor, Venous-Lymphatic Malformations (VLM) or metastasis may involve the orbital apex and extend intracranially, the most common differential for orbito-cranial CVM will be schwannoma [18-20]. Clinically, schwannomas are encapsulated and usually slow-growing and noninvasive, similar to CVM. While deep apical involvement and intracranial extension are unusual, these have been more frequently reported in schwannomas than in CVM [15,20,21]. Conventional imaging alone may not be sufficient in differentiating these two tumors [22]. Nevertheless, several CT and MRI features may still provide useful diagnostic clues and these are summarized in Table 1. In the current series, imaging was suggestive but not uniformly diagnostic, particularly in the absence of dynamic contrast-enhanced MRI. Dynamic Contrast Enhancement (DCE) MRI has been shown to be helpful due to the distinct contrast-enhancement spread patterns and should be strongly considered [22]. Namely, in the early phase of DCE, cavernous venous malformations start enhancement from one point or a portion, while schwannomas start the enhancement from a wide area [22]. However, it should be noted that in some apical cases, particularly with smaller lesions, DCE may not be helpful and the imaging will often remain equivocal.
While the differentiation between CVM and schwannoma may not change management decisions in selected cases, it may influence modality and surgical approaches in others. For instance, selected orbito-cranial schwannomas may be managed with a Transorbital Endoscopic Assisted (TONES) intracapsular excision [23]. The natural history of CVM should be considered, particularly in asymptomatic patients, as some may have stable lesions and intervention can be avoided or deferred [8,24]. Hence, diagnostic accuracy and an MDT (neuroradiologist, radiation oncologist, neurosurgeon and orbital surgeon) meeting to discuss management options are mandatory. Patients should be presented with treatment options and the MDT’s recommendation.
The goal of surgery should be complete excision, as tumor regrowth following incomplete removal is possible [6,25]. Nonetheless, patients should be made aware of the significant rate of collateral damage and morbidity once these lesions are at the apex (and in the cavernous sinus) [2,8,16]. The patient and surgeon should also be prepared for the possibility of incomplete excision [8]. In these cases, the surgeon can consider adjunctive apical decompression, shrinking the tumor with bipolar cautery, tumor decompression or not replacing the posterior orbital roof [8,26]. Postoperative monitoring for progression is then warranted and if detected, radiotherapy is an option [6,27].
Surgical decision-making in orbital cavernous venous malformations is guided by a number of well-established risk factors for visual and neurological morbidity. These include apical location, wedge-shaped configuration, proximity or adherence to the optic nerve and the presence of preoperative optic neuropathy. These factors have been evaluated in recent literature, including a systematic review and large case series and are summarized in Table 2 [28-30]. Notably, the lesions in the current series inherently represented high-risk cases, given their apical location, intracranial extension and association with preoperative visual dysfunction. The surgical approach should therefore be tailored to both lesion location and the anticipated need for safe exposure and control. Consideration should be given to craniotomy, traditional or transorbital incisions, an operative microscope, neuronavigation and an endoscope (TONES) [7,8,16,31-35]. In Cases 1 and 3, the preoperative imaging already suggested high-risk orbito-cranial lesions centered at the orbital apex/SOF and a transcranial cranio-orbital approach was therefore planned from the outset to maximize exposure and control.
By contrast, Case 2 illustrates a different but equally important surgical lesson. Although the initial intent was limited tissue diagnosis, the lesion’s extent and location meant that even a biopsy carried the risk of hemorrhage, poor visualization and inability to safely control the operative field through a restricted corridor. In such cases, a biopsy should only be undertaken if there is a clear preoperative strategy for immediate expansion of exposure should operative findings prove more complex than anticipated. This may include a combined neuro-orbital approach or, in selected medially based apical lesions, consideration of an endoscopic endonasal corridor [14,36,37].
Even when preoperative imaging is suggestive, the full extent of these lesions may only become apparent intraoperatively. Such unexpected extension through the SOF was encountered during surgery in one of our cases and was similarly reported by Rootman, et al. [6]. In our case, complete excision may have been facilitated by the transcranial exposure, whereas Rootman, et al., were unable to achieve complete excision using a lateral orbitotomy approach [6].
Although our series did not include orbito-cranial CVM extending into the optic canal, an endonasal endoscopic approach may be applicable for these lesions, particularly those lying medial to the optic nerve [6,14,36-39]. In these cases, including an experienced skull base rhinologist in the multidisciplinary discussion may be beneficial.
Given the relatively high risk of morbidity associated with surgical excision of apical and orbito-cranial CVMs, Stereotactic Radiotherapy (SRT) may be considered an alternative treatment modality in selected cases, particularly when surgical risk is high or complete excision is not feasible. Treatment modality should ideally be determined in a multidisciplinary setting.
Several reports support the efficacy and safety of radiotherapy for orbital apex CVMs. Gamma Knife and fractionated stereotactic radiotherapy have both been associated with sustained tumor shrinkage, visual stabilization or improvement and low treatment-related morbidity [6,27,40-43]. Radiotherapy (SRT, Gamma Knife and CyberKnife) is also well described as a primary treatment for purely cavernous sinus CVM [44-47]. These data suggest that radiotherapy represents a reasonable alternative in selected high-risk cases, particularly when the anticipated morbidity of surgery is substantial.
Feature | Orbital Cavernous Venous Malformation | Orbital Schwannoma | References |
Location | Intraconal (53.8%); lateral orbit most common | Intraconal (66.7%); mid or posterior orbit (83.4%); superior orbit most common (27%) | [48-50] |
Shape | Round, oval or lobulated; well-defined margins | Multilobulated “beaded” (46.2%), dumbbell (30.8%), oval, fusiform or cone-shaped | [48,50,51] |
T1-Weighted MRI | Hypointense to isointense (80-100%); homogeneous | Isointense to hypointense (85%); heterogeneous appearance (p=0.044) | [48,49,52] |
T2-Weighted MRI | Markedly homogeneous hyperintensity; higher signal than cortex (89.7%) | Heterogeneous hyperintensity; Antoni A (hyperintense on T1, hypointense on T2); Antoni B (hypointense on T1, hyperintense on T2) | [48,49,53,54] |
Characteristic MRI Signs | Linear T2 hypointensity (T2WI, 57.7%); chemical shift artifact (T1WI/T2WI, 89.7%) | Target sign (T2WI/T1WI+Gd, 46.2-76.9%); tail sign (T2WI, 46.2%); fascicular sign (T2WI, 35.8%) | [48,50,51,54,55] |
Dynamic Contrast Enhancement Pattern | Nodular early enhancement; progressive filling from single starting point (62.1%); persistent or plateau time-intensity curve | Diffuse early enhancement from wide area; heterogeneous enhancement; variable time-intensity curve | [48,49] |
Enhancement Characteristics | Progressive contrast enhancement (93.9%); homogeneous filling in late phase | Peripheral (ring) enhancement (29%); homogeneous (26%) or heterogeneous (42%) enhancement | [49,50] |
Diffusion-Weighted Imaging | Non-restricted diffusion (high ADC) | Non-restricted diffusion (high ADC) | [48,49] |
CT Density | Higher (56 HU) | Lower (40 HU) | [48] |
Bone Changes | Smooth expansion or remodeling possible | Bony remodeling (100% on CT); smooth expansion of foramina | [48,51,56] |
Cystic Degeneration | Less common | Present in 46.2% of cases | [51,57] |
Table 1: Radiological features of orbital cavernous venous malformation versus shwannoma.
Risk Factor Category | Specific Risk Factor | Effect/Outcome | Statistics | References |
Anatomical/Location | Apical location | Predictor of poor visual outcome on multivariate analysis; ~30% risk vs ~5% for “free” retrobulbar lesions | OR 4.9, p=0.036 | [29,30] |
Wedge-shaped apical lesions | Associated with complete visual loss (NLP); 58% of NLP cases had wedged apical lesions | – | [30] | |
Location below optic nerve | Increased risk of visual loss | RR 3.3, p=0.007 | [30] | |
Lateral quadrant location | Increased risk of permanent tonic pupil (3% incidence) | p=0.011 | [28] | |
Strong adherence to apical structures/optic nerve | Higher risk of postoperative vision loss | – | [29] | |
Lesion Characteristics | Fibrous masses | Strongest predictor of poor visual outcome on multivariate analysis | OR 10.0, p=0.035 | [30] |
Tumor volume >1100 mm³ | Associated with choroidal folds | p=0.001 | [28] | |
Preoperative Clinical | Preoperative visual loss | Poor visual prognosis | – | [29] |
Relative afferent pupillary defect (RAPD) | Increased risk of visual loss | RR 2.9, p=0.011 | [29,30] | |
Optic disc abnormality | Poor visual prognosis | – | [29] | |
Choroidal folds | Poor visual prognosis | – | [29] | |
Intraoperative | Prolonged vascular handling/traction on optic nerve | Higher risk of vision loss; central retinal artery occlusion most common mechanism | – | [29] |
Low intraoperative diastolic BP (<50 mmHg) | Increased risk of visual loss | RR 2.8, p=0.007 | [29,30] |
Table 2: Risk factors for morbidity following surgical excision of orbital cavernous venous malformations.
Year | Number of Cranial-Extending Lesions | Extension Pattern | References |
1983 | 1 | Bone involvement (intraosseous) | [11] |
1998 | 2 | Apex → cavernous sinus via superior orbital fissure | [5] |
1998 | 1 | Apex → Superior orbital fissure | [7] |
2004 | 1 | Apex → intracranial via superior orbital fissure | [58] |
2006 | 1 | Bone erosion | [12] |
2008 | 1 | Apex → cavernous sinus via superior orbital fissure | [13] |
2010 | 2 | Apex → cavernous sinus via superior orbital fissure | [8] |
2012 | 3 | 1 Apex → Superior orbital fissure 2 Apex → cavernous sinus via superior orbital fissure | [6] |
2015 | 1 | Apex → cavernous sinus via superior orbital fissure | [31] |
2020 | 1 | Bone involvement (intraosseous) | [59] |
Table 3: Previous reports of orbito-cranial cavernous venous malformations.
In conclusion, the current small series focuses on the surgical management of orbito-cranial cavernous venous malformations, a rare and complex presentation of a common orbital lesion. Using modern imaging and involving experienced neuro-radiologists is highly likely to correctly diagnose an orbito-cranial CVM or favor it over the differential diagnoses. A multidisciplinary discussion to determine treatment modality is then advisable. Consideration should be given to radiotherapy versus surgery and the patient should be involved in treatment choice. If surgery is favored, careful neurosurgical and orbital planning is needed to choose the appropriate approach. Patients should be counseled regarding the incidence of collateral nerve damage and the possibility of incomplete excision.
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
This research did not receive any specific grant from funding agencies in the public, commercial or non-profit sectors.
Permission was obtained from the publisher (copyright owners)[10] for the re-use of some of the images in this work.
Not applicable.
This study received approval from the Central Adelaide Local Health Network (CALHN) Human Research Ethics Committee (HREC) and CALHN Research Services (approval number 14862) and adhered to the tenets of the Declaration of Helsinki.
Requirement for patient consent was waived by the ethics committee.
YS contributed to study conception, data interpretation, and drafting of the manuscript. DS contributed to study conception, data interpretation, and data acquisition. VJ contributed to study conception and data acquisition. TD, SS, and JAN contributed to data acquisition. All authors contributed to manuscript revision and approved the final version.
https://www.issva.org/classification
Yinon Shapira1,2*![]() , Valerie Juniat3, Tarjani Dave4, Stephen Santoreneos5, Jeffrey A Nerad6, Dinesh Selva7
, Valerie Juniat3, Tarjani Dave4, Stephen Santoreneos5, Jeffrey A Nerad6, Dinesh Selva7
1Department of Ophthalmology, Carmel Medical Center, Haifa, Israel
2The Bruce and Ruth Rappaport Faculty of Medicine, Technion-Israel Institute of Technology, Haifa, Israel
3Department of Ophthalmology, Sussex Eye Hospital, Brighton, UK
4Ophthalmic Plastic Surgery Service, L V Prasad Eye Institute, KAR Campus, Hyderabad, Telangana, India
5Department of Neurosurgery, Royal Adelaide Hospital, Adelaide, South Australia, Australia
6Cincinnati Eye Institute, Cincinnati, Ohio, USA
7Department of Ophthalmology, Royal Adelaide Hospital and South Australian Institute of Ophthalmology, Adelaide, South Australia, Australia
*Correspondence author: Yinon Shapira, Department of Ophthalmology, Carmel Medical Center, Haifa, Israel; Email: [email protected]


{kind=link}